Dyslipidemia
Winter 2024 / 2025
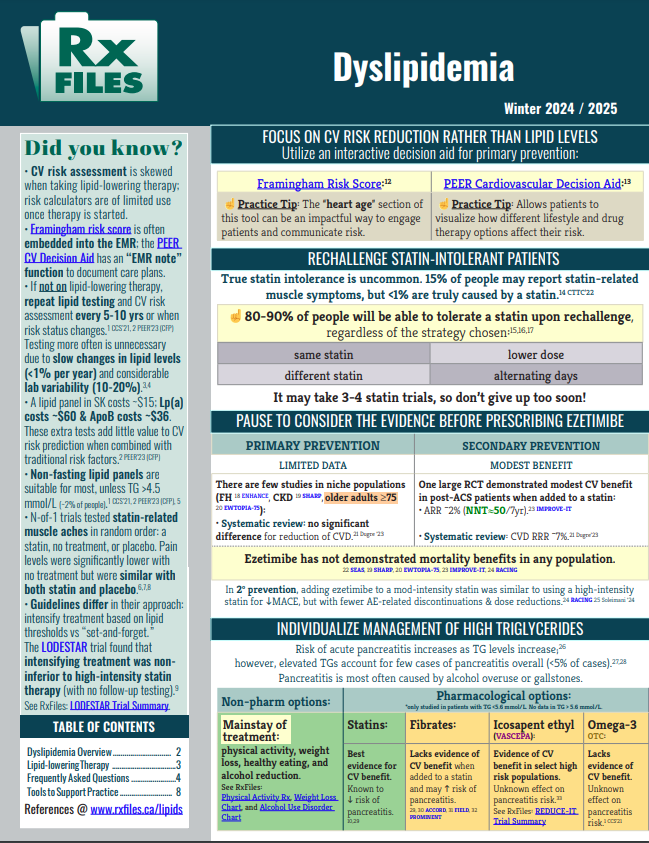
HIGHLIGHTS
· Focus on cardiovascular risk reduction rather than on lipid levels.
· Use an interactive decision aid for primary prevention.
· Rechallenge statin-intolerant patients.
· Consider the evidence before prescribing ezetimibe.
· Individualize the management of high triglycerides.
Visit: www.rxfiles.ca/lipids